Humeral fractures with and without bias
According to statistics, 7% of fracturesfalls on the humerus. Such damage occurs mainly due to falls and shocks. Fractures of the humerus are possible in different parts of it, which is accompanied by various symptoms and sometimes requires separate approaches to treatment.
Anatomical structure
The humerus bone is divided into three parts: the body or diaphysis is the middle part, and the ends are called epiphyses. Depending on the location of the lesions, they indicate fractures of the upper, middle or lower part of the shoulder. The upper section is also called the proximal, and the lower one is called the distal one. Diaphysis divided into a third: upper, middle and lower.

In turn, the epiphyses have a complex structure,because they enter the joints and keep the muscles. In the upper part of the humerus is a semicircular head and an anatomical neck - the area immediately below the head. They and the articular surface of the scapula come into the shoulder joint. Under the anatomical neck there are two tubercles, which serve as the place of attachment of muscles. They are called a large and small tubercle. Even further, the bone narrows, forming the so-called surgical neck of the shoulder. The lower part of the humerus is represented immediately by two articular surfaces: with the radius of the forearm articulated the head of the condyle, which has a rounded shape, and the humerus block leads to the ulnar bone.
Basic types of fractures
Classification of fractures is conducted on several parameters. On the one hand, fractures of the humerus are grouped by location, i.e. by departments. So, there is a fracture:
- in the proximal (upper) part;
- diaphysis (middle section);
- in the distal (inferior) department.
In turn, these classes are further split into varieties. In addition, there may be a fracture at once in several places within one department or in neighboring ones.
On the other hand, you can divide the damage intofractures with and without bias, as well as isolate fragmented (comminuted) fractures. There are also traumas that are open (with damage to soft tissues and skin) and closed. At the same time, the most prevalent in everyday life.
Specification of the type of fracture by department
A fracture in the proximal part can be divided intointraarticular or extraarticular. With intraarticular (epigastric), the head or the anatomical neck of the bone can be damaged. The extra-articulate is divided into a fracture of the humerus of the humerus and a fracture of the lower surgical neck.

If the diaphysis is damaged, several subspecies are also identified: fracture of the upper third, middle or lower. Also important is the character of bone fracture: oblique, transverse, helical, comminuted.

The distal department may also sufferdifferently. It is possible to distinguish epicondylar extraarticular fracture, as well as fractures of condyles and block, which are related to intraarticular fractures. A deeper classification highlights the flexor and extensor epicondylar, as well as the overcross, intercondylar, or T-shaped and fractured condyles.
Prevalence
In everyday life, because of falls and blows, the majority suffersthe surgical neck of the upper part, the middle third of the diaphysis or the epicondyle of the lower part of the humerus. Closed fractures predominate, but very often they can be offset. It should also be noted that several types of fractures can be combined simultaneously (more often within the same department).
The fracture of the head of the humerus, anatomical andSurgical necks are most common in the elderly. The lower part often suffers in children after an unsuccessful fall: they are not uncommon between the intercondylar and the overcrossing fractures. The body of the bone (diaphysis) is subject to fractures quite often. They occur when striking the shoulder, as well as when falling on the elbow or straightened arm.
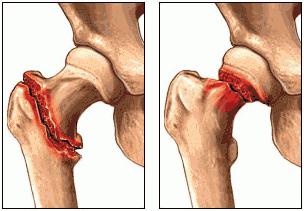
Fractures of the proximal part
To intraarticular carry fracture of the headhumerus and immediately behind the anatomical neck. In the first case, a comminuted fracture can occur, or a dislocation can be observed additionally. In the second case, a fractured fracture may occur, when the fragment of the anatomical neck is inserted into the head and can even destroy it. In case of direct injury without detachment, the fragment can also be fragmented, but without significant displacement.

Also to proximal injuryThey include a fracture of the large tubercle of the humerus and of the small one: peri-humpy and detachment of tubercles. They can arise not only when falling on the shoulder, but also with too strong a sharp contraction of the muscles. Fracture of the humerus of the humerus can be accompanied by fragmentation without significant displacement of the fragments or by moving it to the acromedial process or down and out. Such damage can occur with direct injury or dislocation of the shoulder.
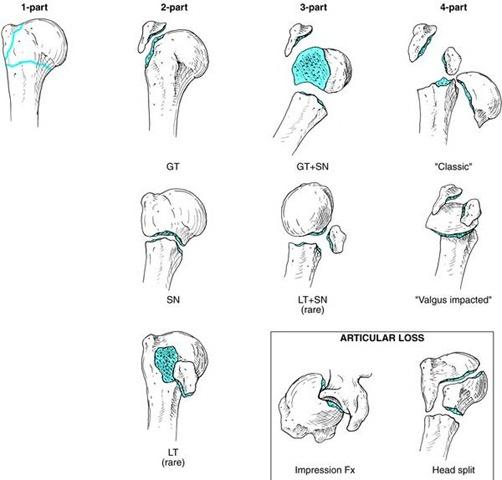
The most frequent is a fracture of the surgicalneck of the shoulder. The reason is most often falling. If the hand at the time of injury was withdrawn or brought, then an abduction or an adduction bone fracture is noted, with the middle position of the limb, a fractured fracture can result, when the distal fragment is inserted into the upper part.
Fracture can be simultaneously in severalplaces. The bone is then divided into two or four fragments. For example, fracture of the anatomical neck may be accompanied by the detachment of one or both tubercles, fracture of the surgical neck should be supplemented with a head fracture, etc.
Symptoms of a fracture in the upper part of the shoulder

Intra-articular fracture is accompanied by edemadepartment or even a hemorrhage in the joint. Visually, the shoulder increases in volume. Painful is the pressure on the head. Fracture of the neck of the humerus gives pain in circular movements and palpation. When punctured fracture of the surgical neck, movements in the shoulder joint may not be disturbed. If there is an offset, then the limb axis may change. In the joint area, there may be a hemorrhage, swelling, or just a swelling. When a characteristic bone protrusion appears on the anterior anterior surface of the shoulder, one can speak of an adduction fracture, and if there is a deviation, this indicates an abduction.
Also, a surgical fracture of the humerus cancause pathological mobility. Fractures with large displacement or fragmentation can block active movements, and even a slight axial load and passive movements cause severe pain. The most dangerous is the option in which fracture of the neck of the humerus occurs with additional damage, jamming, squeezing of the vascular bundle. Squeezing this beam causes swelling, decreased sensitivity, venous stasis and even paralysis and hand paresis.
Fracture of the large tubercle of the humerus gives pain in the shoulder, especially when turning the arm inside. Movements in the shoulder joint are broken, become painful.
Symptoms of a diaphysis fracture
Humeral fractures in the diaphysis regionoccur quite often. There is swelling, pain and uncharacteristic mobility at the site of injury. The fragments can move in different directions. Hand movements are violated. Hemorrhages are possible. Fractures with a strong bias are visible even to the naked eye by deforming the shoulder. If the radial nerve is damaged, it is impossible to unbend the hand and fingers. However, to study the nature of the damage, an X-ray photograph is needed.
Fractures in the distal part and their symptoms
Fractures of the distal department are divided into extra-articular(supracondylar extensor or flexor) and intraarticular (condylar, supra-locomotor, fractures of the head elevation or humerus block). Violations in this department lead to deformity of the elbow joint itself. There is also pain and swelling, and the movements become limited and painful.

Supracondylar flexion occurs afterfalls on the bent arm, lead to swelling, swelling above the injury site, pain sensations and visible to the naked eye extension of the forearm. Extensor muscles appear when the hand is over-folded when it falls, visually shortens the forearm and is accompanied by pain and swelling. Such fractures can also be combined with simultaneous dislocation in the joint.
Fractures of the external condyle often accompanyfalling on a straight elongated arm or direct injury, and the internal breaks when falling on the elbow. There is swelling in the elbow area, pain, and sometimes a bruise or a hemorrhage in the joint itself. Movement in the elbow joint is limited, especially with hemorrhage.
Fracture of the head elevation can appear when falling on a straight arm. Also, movement in the joint is limited and pain arises. As a rule, this is a closed fracture of the humerus.
First Aid and Diagnosis
If there is a suspicion of a fractureThe limb must be correctly fixed in order to prevent the deterioration of the situation. You can also use analgesics for pain relief. After this, the victim should be taken to the hospital as soon as possible for accurate diagnosis and professional assistance.
Diagnose the fracture can be on the abovesymptoms, but the final results can be obtained only after radiography. Usually, images are taken in different projections to clarify the full picture. Fractures of the humerus are sometimes implicitly expressed, they are difficult to distinguish from dislocations, sprains and bruises, which require other treatment.
Treatment of minor fractures
Fracture of humerus without displacement requiresimmobilization of the limb with gypsum or with a diverting bar. Complications here are extremely rare. If there is an insignificant displacement, reposition is performed followed by immobilization. In some cases it is sufficient to install a removable linget, others require a full fixation.
Minor fractures of the proximal partallow already in three days to perform UHF and magnetotherapy, and after 7-10 days to start developing the elbow and wrist joints, perform electrophoresis, UV, massage and ultrasound. After 3-4 weeks, gypsum, longite or special fixatives are replaced by a bandage, continuing exercise therapy and procedures.
Recovering deleted fragments without an operation
More serious injuries, such as fracturesurgical cervix or fracture of the humerus with displacement, require reposition, plaster bandage and regular X-ray control in a hospital setting. Gypsum can be applied for 6-8 weeks. It is necessary to move the brush and fingers from the next day, after 4 weeks passive movements of the shoulder joint can be performed, helping with a healthy hand, then moving to active movements. Further rehabilitation includes exercise therapy, massage and mechanotherapy.
Need for surgical interventions
In some cases, repositioning is not possible due tostrong fragmentation or simply does not give the desired results. If such a fracture of the humerus is present, treatment is required with surgical intervention to achieve the alignment of the fragments. Strong displacements, fragmentation or fragmentation, instability of the fracture site may require not just repositioning, but also osteosynthesis - fixing debris with spokes, screws, plates. For example, fracture of the neck of the humerus with complete divergence of fragments requires fixation with the Kaplan-Antonov plate, spokes, Vorontsov or Klimov beam, pin or rod, which avoids the appearance of angular displacement during adhesion. The fragments are retained until matched by screws or Ilizarov apparatus. Skeletal and adhesive plasty traction is additionally used in fractured fractures of the lower part, after which a tire is applied and therapeutic gymnastics is performed.

Fractures of epicondyles without displacement require wearingplaster bandages for 3 weeks. Displacement may require surgery. The condylar (intercondylar and over-cramped) fractures are often accompanied by a displacement of the fragments and are operated on. The reposition in this case is made open to make sure of restoring the correct position of the articular surfaces and to perform osteosynthesis. Then apply restorative treatment in the complex.
Treatment of complicated fractures
Fracture of humerus with displacement,accompanied by damage to the radial nerve, requires comparison of bone fragments and conservative treatment of the nerve itself. Fracture is immobilized, supplemented with drug therapy, so that the nerve itself can be regenerated. Later they connect exercise therapy and physiotherapy. But if the functionality of the nerve is not restored after a few months, then surgery is performed.

In the most difficult cases, when the bones are toothe fragments can be removed, after which a prosthesis is required. In the shoulder joint, an endoprosthesis is used instead of the head. With excessive damage to the tubercle, the muscles can be sewn directly to the humerus.
Treatment of any fracture requires compliance with allrecommendations of specialists, as well as a serious approach to rehabilitation. Immobilization and complete rest of the damaged surface are replaced with certain loads over time. Courses of physiotherapy, physiotherapy, massage and similar procedures can be appointed repeatedly with some interruptions until complete recovery. It is also important to conscientiously implement all the prescriptions for rehabilitation at home and be careful of re-injury.