Pulmonary vein. Abnormal drainage of pulmonary veins
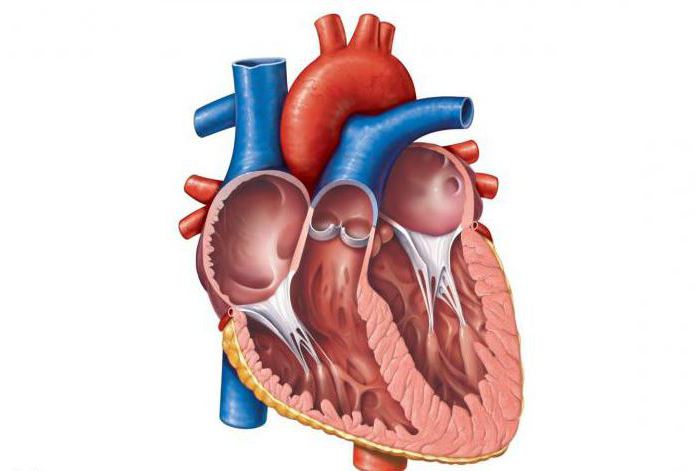
The pulmonary vein (pictured below) is a vessel that brings arterial blood enriched with oxygen in the lungs to the left atrium.
Starting from the pulmonary capillaries, these vesselsmerge into larger veins, which are sent to the bronchi, then to the segments, to the lobes, and in the lungs' gates form large trunks (two from each root) that go horizontally to the upper part of the left atrium. In this case, each of the trunks penetrates into a separate hole: the left - on the left side of the left atrium, and the right from the right. Right pulmonary veins, following to the atrium (left) cross the right atrium (its posterior wall) transversely.
Upper pulmonary (right) vein
It is formed by segmental veins from the segments of the middle and upper lobes of the lung.
- R.apicalis (branch apical) - is represented by a short venous trunk, which is located on the upper lobe (its medial surface) and carries blood from the segment of the apex. Before penetrating the upper pulmonary right vein, it is often combined with a segmental (posterior) branch.
- R. posterior (the branch rear) performs the collection of blood from the posterior segment. This branch is the largest vein of all veins (segmental), located in the upper lobe. In this vessel, several parts are distinguished: an intrasegmentary segment and a sub-lobe segment that collects blood from the interlobar surface in the region of the oblique fissure.

- R.anterior (Branch front) collects blood from the upper lobe (its anterior segment). In some cases it is possible to combine the posterior and anterior branches (then they fall into a common trunk).
- R.lobi medii (middle branch) receives blood from the segments of the right lung (its middle lobe). In some cases, this vein takes the form of one trunk and empties into the upper right pulmonary vein, but more often the vessel is formed from two parts: medial and lateral, which drain respectively the medial and lateral segments.
Lower pulmonary (right) vein
This vessel receives blood from the lower lobe (its 5 segments) and has two main inflows: the basal common vein and the upper branch.
Upper branch
It lies between the basal and upper segments. Formed from the additional and main veins, it follows forward and downward, passing behind the segmental apical bronchus. This branch is the uppermost of all that flows into the lower right pulmonary vein.
In accordance with the bronchus, the main vein contains three inflows: lateral, upper, medial, which are mostly intersegmented, but can also be intersegmented.

Due to the additional vein, the blood flow from the upper segment (its upper part) to the subal region of the segmental posterior vein of the upper lobe (its posterior segment) is carried out.
Basal common vein
It is a short venous trunk formed by the fusion of the lower and upper basal veins, the main branches of which lie much deeper than the anterior lobar surface.
Basal upper vein. Formed by merging the largest of the basal segmental veins, as well as veins that carry blood from the medial, anterior and lateral segments.
Basal lower vein. Adjoins to the basal common vein from the side of its posterior surface. The main inflow of this vessel is the basal posterior branch, which collects blood from the basal posterior segment. In some cases, the basal lower vein may approach the basal superior vein.
ADLV
It is a congenital pathology of the heart, in which a non-anatomical entry of pulmonary veins into the atrium (right) or those entering the last hollow veins is revealed.

This pathology is accompanied by frequentpneumonia, fatigue, dyspnea, lag in physical development, heart pain. As diagnostics apply: ECG, MRI, radiography, heart probing, ultrasound, ventriculo- and atriography, angiopulmonography.
Surgical treatment of vice depends on its type.
General information
ADLV - congenital malformation and is about 1.5-3.0% of heart defects. Most of them are observed in male patients.
Most often this defect is combined with an oval(open) window and defects of the septum between the ventricles. Slightly less often (20%) - with arterial common trunk, left heart hypoplasia, DMF, dextrocardia, Fallot tetrad and transpositions of the main vessels, common ventricle of the heart.
In addition to the aforementioned defects, ADLV oftenis accompanied by extracardiac pathology: umbilical hernia, defects in the formation of the endocrine and bone systems, intestinal diverticula, horseshoe kidney, hydronephrosis and polycystic kidney disease.
Classification of abnormal drainage of pulmonary veins (ADLV)
In the case of the confluence of all veins in a large circleblood circulation or in the right atrium, this vice is called complete abnormal drainage, if one or several veins enter into the above structures, then such a vice is called partial.
In accordance with the level of confluence, several variants of the defect are distinguished:
- Option one: supracardiac (supracardial). Pulmonary veins (as a common trunk either separately) flow into the hollow upper vein or its branches.
- Option two: cardiac (intracardial). Drains the pulmonary veins into the coronary sinus or right atrium.
- Option three: sub-cardiac (infra- or subcardial). Pulmonary veins enter the portal or hollow lower vein (much less often into the lymphatic duct).
- Fourth option: mixed. Pulmonary veins enter into different structures and at different levels.
Features of hemodynamics
In the prenatal period, this defect as athe rule does not appear, due to the peculiarities of the fetal circulation. After the birth of the baby manifestations of hemodynamic disorders are determined by the variant of the defect and its combination with other congenital anomalies.
In case of total abnormal drainage, hemodynamic disturbances are expressed by hypoxemia, hyperkinetic overload of the right heart and pulmonary hypertension.
In the case of partial drainage, hemodynamics is similar tosuch with ASD. The predominant role in the disorders belongs to the abnormal venous-arterial discharge of blood, which leads to an increase in the blood volume in a small circle.
Symptoms of abnormal drainage of pulmonary veins
Children with this defect often suffer from repeated SARS and pneumonia, they have cough, low weight gain, tachycardia, dyspnea, heart pain, light cyanosis and rapid fatigue.

In the case of overt pulmonary hypertension, at a small age, heart failure, pronounced cyanosis and a heart hump occur.
Diagnostics
The picture of auscultation with ADLV is similar to ASD, that is, systolic non-rough noise is heard in the area of the projection of the arteries of the veins (pulmonary veins) and the splitting of the 2nd tone.
- On ECG signs of an overload of the right heart, deviation of the EOS to the right, blockade (incomplete) of the right leg of the bundle of Giss.
- In phonographics, signs of ASD.
- On radiography, the increase in the pattern of the lungs, the swelling of the pulmonary artery (its arches), the expansion of the heart boundaries to the right, the "Turkish saber" symptom.
- Echocardiography.
- Sounding of the heart cavities.
- Phlebography.
- Atriography (right).
- Angiopulmonography.
- Ventriculography.

Differential diagnosis of this defect should be carried out with:
- Lymphangiectasia.
- Atresia of the aortic / mitral valve.
- Transposition of blood vessels.
- Stenosis is mitral.
- Stenosis of the right / left pulmonary veins.
- Atrial at heart.
- Isolated ASD.
Treatment
Types of surgical treatment of partial drainage are determined by the variant of the defect, the size and location of the ASD.

The interatrial message is eliminated byplastic or suturing. Breasts up to three months of age, who are in critical condition, are palliative (closed atrioseptotomy), which is aimed at expanding interatrial communication.
The total radical correction of the defect (total form) involves several manipulations.
- Bandaging the pathological communication of blood vessels with veins.
- Pulmonary veins isolation.
- Closure of the ASM.
- Formation of anastomosis between the left atrium and pulmonary veins.
The consequence of such operations may be: an increase in pulmonary hypertension and a syndrome of sinus node insufficiency.
Forecasts
The prognosis for the natural course of this defect is unfavorable, as 80% of patients die during the first year of life.
Patients with partial drainage can live up to the age of thirty. The death of such patients is most often associated with pulmonary infections or heart failure.
The results of surgical correction of the defect are more often satisfactory, but among newborns the lethality during or after the operation remains high.